How our Emotions can Influence the Pain We Experience
Posted by Phil Heler on December 12, 2023Our Emotions and Performing Complex Demanding Tasks can reduce Neurological Pain Activation and the Pain we feel!
Someone once said that ‘pain is a near-universal part of the human condition’. But what exactly is pain, how is it defined? This is a question that science has been wrestling with for some time. Writers and musicians have spun tales and crafted songs intertwining physical and emotional pain for centuries. Bob Dylan, famous for his verbal dexterity, told us ‘Behind every beautiful thing, there’s some kind of pain.’
The author C.S. Lewis (who wrote ‘The Lion, The Witch and the Wardrobe’ in 1950) wrote that ‘Pain insists upon being attended to. God whispers to us in our pleasures, speaks in our consciences, but shouts in our pains. It is his megaphone to rouse a deaf world.’ Yet pain is complex. Pain and strong physical responses can be evoked by powerful emotions such as fear, emotional rejection, or grief.

From my own experiences in the last 20 years, I have realised that pain certainly does instinctually yearn to be communicated. This is frequently expressed by people on the receiving end of god’s megaphone when they visit my clinic. Verbal expressions of pain range from a simple ‘ouch’ to some more interesting fruity expletives as people hobble through our clinic door. It must be said that a healthy bit of swearing when you stub your toe does no end of good and feels very cathartic!
One of the things I most struggle with, as does modern medicine in general, is how do you interpret and quantify a person’s pain? This is quite an important point in my line of work as I partly rely on someone’s own subjective assessment of their condition to give an indication of response to treatment.
But pain, as I mentioned earlier, is both a physically and emotionally richly complicated experience, so how does someone rate their pain using a basic scale that simplifies this and rolls it all up into a single number. Pain is by nature a very subjective experience and it is hard to condense it into an almost meaningless figure or abstract pain rating.
Modern medicine has always used a system called the Visual Analogue Scale (VAS). The use of this system is generally attributed to Hayes and Patterson who invented it in 1921. Examples of the VAS are given below.
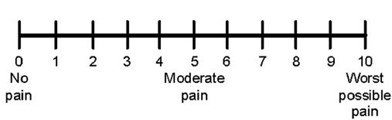

It does seem odd that this is still utilised 100 years later. By its very nature this system is problematic, the most obvious point being that you must rate your pain experiences anywhere between zero (meaning no pain) to 10 (maximum pain imaginable). This somewhat antiquated scale does not adequately capture the complex phenomenon of pain. Pain is influenced by a multitude of factors including duration, extent, characteristics, environmental, developmental, genetic, and of course psychological.
In terms of neuroscience and anatomy the origin of pain is difficult to source. Many of our senses like vision (processed in the visual cortex) and hearing (processed in the temporal lobe) can be traced back to specific tissues in our brain. This not the case with pain.
What is clear is that pain is closely linked to our thoughts and emotions and involves a diverse neurological network. For instance, there is evidence to suggest that people report much less pain intensity if they are given what is known as an ‘interference task’ to perform.
An interference task given is predetermined, is typically cognitively demanding, and known to stimulate a wide network of brain regions. A study done in 2002 (Bantick et al) undertook neuroimaging techniques on participants while they performed interference tasks.
The study objective was to determine how this influenced areas in the brain which were involved in pain perception. The study concluded that pain activation centres and key areas involved in the neural pain matrix became much less active when subjects performed interference tasks. Pain became heavily modulated when a participant’s attention was shifted elsewhere to other neurological regions needed to process and perform tasks. This suggest there is some form of neurological hierarchy.

Another study, also using neuroimaging techniques, suggested that even listening to music as an interference task can significantly reduce postoperative pain in patients by modulating their pain centres (Goodet et al 1999). However, conversely if there is nothing else competing for our attention (i.e. no interference) pain centres increase their activity, and more pain is perceived.
Interestingly there is also clinical evidence to suggest that mood and physical pain have a relationship although very little is known about the cognitive and neural mechanisms. A study performed in 2010 demonstrated that our mood will influence the level of pain that we feel.
This investigation scanned real time neural activity of 20 healthy volunteers to examine the interaction between mood and pain (pain was provided by a heat stimulus! Ouch!). The study proved conclusively that changes in emotion regulation mechanisms (meaning a low mood) led to stimulation in pain activation centres. The results informed how depressed mood and chronic pain can co-occur clinically. Emotions however do more than just modulate pain.
Another investigation from 2011 proved the experiences of social rejection and physical pain activate the same regions of the brain. This not so happy study was entitled ‘Social rejection shares somatosensory representations with physical pain’. It was demonstrated that when rejection is strongly elicited—sadly by having participants who recently had an unwanted break-up stare at a photograph of their ex-partner as they think about being rejected—regions of the brain that support physical pain become active.
So, there is an overlap between social rejection and physical pain and these results give new meaning to the idea that rejection literally ‘hurts’. Rejection and physical pain are identical not only in the way that they are distressing—but they share a common somatosensory representation as well.
Why is all this important? My job is to deal with pain and discomfort and to understand the emotional aspects of pain helps me do my job properly and empathise. Many chronic pain issues especially have an underlying mood alteration such as anxiety, depression, lack of sleep and energy, and generalised diffuse pain states. We all go through difficult times at one point or another in our lives and have certainly been there. It is important to understand anxiety and depression can worsen a person’s experience of pain, dull the efficacy of opioids and heighten the risk of chronic pain.