Polymyalgia Rheumatica (or PMR). If you are over 50 years Old this is Something you should know About
Posted by Phil Heler, MD on September 28, 2018Polymyalgia Rheumatica is an inflammatory rheumatological syndrome that manifests as pain and morning stiffness involving the neck, shoulder girdle, and/or pelvic girdle in individuals older than age 50 years. Peripheral musculoskeletal involvement may also be present’
OVER 50? You should know about Polymyalgia rheumatica (or PMR).
Polymyalgia rheumatica (or PMR) is a condition which we often see in clinic because it presents in a very similar way to a sudden onset of neck or shoulder or hip pain. Polymyalgia Rheumatica does respond well to treatment but it is important to appreciate the difference between it and general aches and pains. Furthermore it is quite often missed by GP’s. This is significant because PMR can come with complications in a low percentage of cases. It’s estimated 1 in every 1,200 people in the UK develop the condition every year. However I have to say I personally feel the incidence rate is possible higher. The cause of PMR is unknown, but a combination of genetic and environmental factors is thought to be responsible.
The official definition of PMR is as follows. ‘PMR is an inflammatory rheumatological syndrome that manifests as pain and morning stiffness involving the neck, shoulder girdle, and/or pelvic girdle in individuals older than age 50 years. Peripheral musculoskeletal involvement may also be present’.
So what is the difference between Polymyalgia Rheumatica and a typical musculoskeletal (MSK) complaint?
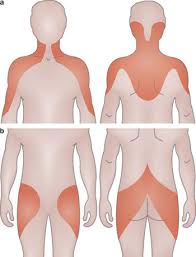
PMR is rarely seen in patients younger than 50. Ladies are twice as likely to develop PMR as men. It is usually accompanied by painful stiffness, which is often worse in the morning, especially in your shoulders and hips and in many cases it can affect both left and right sides at the same time. Polymyalgia Rheumatica appears suddenly over a week or two and is unusual in that it is often worse when resting and improves with activity (i.e. the opposite of an MSK presentation) Unlike a normal MSK presentation it can also be accompanied by;
- feeling unwell
- a slight fever
- weight loss
- overwhelming tiredness
- feeling low, anxious or depressed.
It is very important to appreciate that About 15% to 20% of patients with PMR have giant cell arteritis (GCA). In GCA the arteries in the head and neck become inflamed.
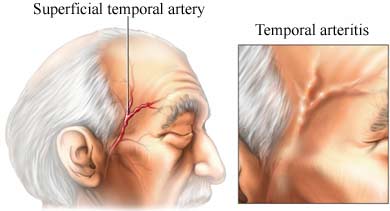
What you Should Know about Giant Cell Arteritis
Symptoms of giant cell arteritis include:
•a severe headache that develops suddenly – your scalp may also feel sore or tender
•pain in the jaw muscles when eating
•problems with sight – such as double vision or loss of vision
If you have any of these symptoms, it is important to contact your GP immediately,
Diagnosis is made via a case history and with blood tests which look at the erythrocyte sedimentation rate (ESR) and or the C-reactive protein (CRP) test.
Both of these blood tests give a broad indication that there is some inflammation going on in the body.
Many conditions cause the ESR and CRP to change, so a number of other tests may have to be performed to exclude those that can be mistaken for PMR.
Once confirmed, PMR is treated using corticosteroids and rapid improvement often occurs within 24 to 72 hours with a low-dose prednisolone. You’ll initially be prescribed a moderate dose of prednisolone, which will be gradually reduced over time.
Most people with PMR will need to take a course of corticosteroid treatment that lasts 18 months to two years to prevent their symptoms returning.